I think that all Australians, regardless of where they live, should have access to accurate medical diagnoses and interventions. When it comes to basic access to specialist care in remote and rural locations, the playing field really needs to be levelled.
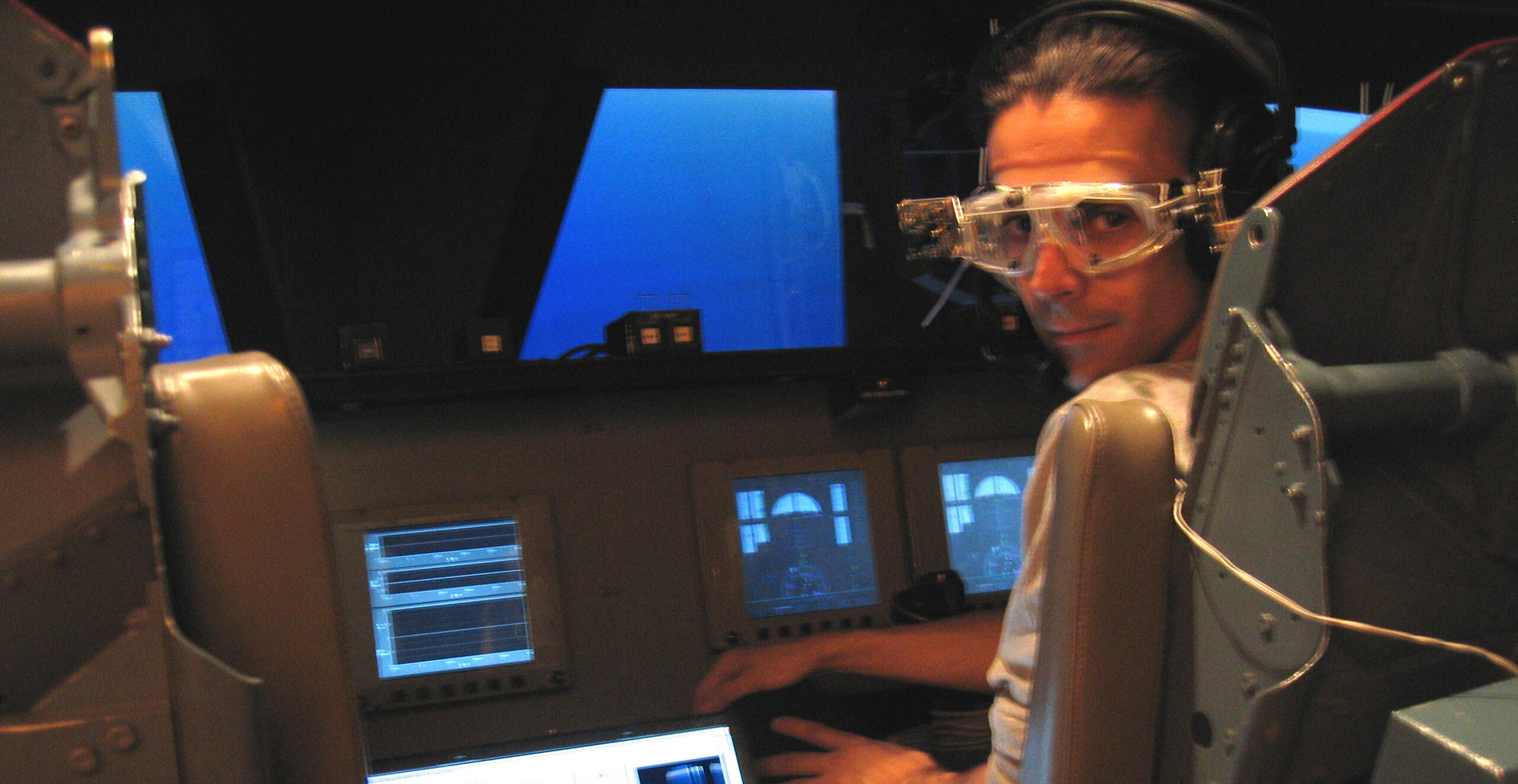
With an exciting career that includes a stint at NASA, Dr Hamish MacDougall’s professional career has been defined by a string of inventions fuelled by curiosity and a desire to improve neurological conditions. He has now joined the Bionics Institute, where he is working on an extended reality (XR) device solution for the diagnosis of neurological conditions.
We sat down with Hamish for a conversation about his research.
Why did you join the Bionics Institute?
What really drew me to the Bionics Institute is how different it is to other organisations. Because my research is dependent on being able to get devices out into the public, into the lives of people who need them, I wanted to work somewhere that not only understood the value and necessity of commercialisation, but also had the experience and the success to make it happen.
At the start of my career, I thought science just about the endless cycle of creating a gadget and publishing a paper about it, then putting the gadget in a box on a shelf and starting the process all over again. But, seeing the gaps that exist in healthcare makes you realise just how valuable it is to get those devices off the shelves and into the world.
Commercialisation is the only real pathway for doing that, getting a gadget from a bench in the lab into tens of thousands of clinics. I can’t physically make thousands of prototypes; you need a commercial partner for that. The Bionics Institute really understands that pathway, and that’s why I chose to come here.
Tell us a bit about what you’re working on right now.
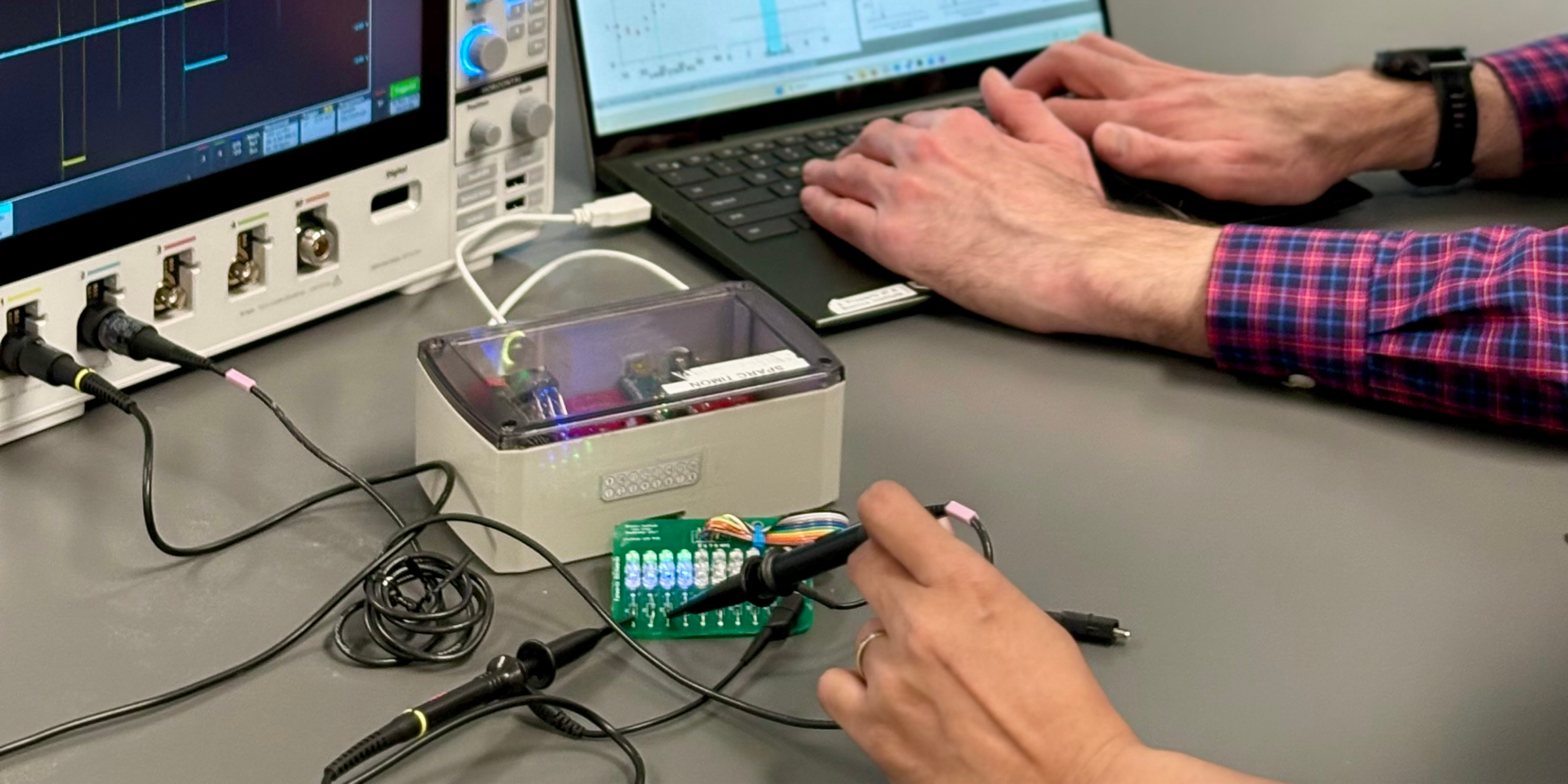
My main project at the moment uses Extended Reality (XR) – the umbrella term that includes virtual reality, mixed reality and augmented reality. I have developed a XR headset which is capable of administering a huge variety of tests and can be remotely accessed from anywhere.
What this means is, we can send this headset out to, say, a remote clinic in rural NT, and the GP out there can put this headset on a patient who’s having a vision or neurological problem. The GP can then go and make himself a coffee, or do some paperwork for half an hour, while a specialist working out of a hospital here in Melbourne can communicate with the individual and run tests in real time.
The tests will show up on the screen for the patient to follow with their eyes, and the data captured about their eye movements can be sent back to the specialist in real time for analysis.
It means we can move it away from subjective, conversational diagnosis and into real, definitive data that clinicians can use for accurate diagnosis.
How does it differ from what currently exists in clinics?
The first difference is cost, which is obviously a concern. The current options that can do a similar thing are around $100,000. Second is the testing capabilities. These goggles can do many different tests, which has the potential to open up lots of new avenues. Ophthalmologists, for example, don’t currently have anything like this that they can use for testing and analysis. And third is, of course, the portability.
When you put all three differences together, that intersection is where the possibilities really open up. That’s what I find so exciting. Imagine being able to send these out on every plane with the Royal Flying Doctor Service, or the Fred Hollows Foundation. We’re talking about something that fits in a case not much bigger than a lunchbox. A social worker could throw it in the passenger seat of their car when they go out to visit people. The possibilities are endless.
What makes this so important?
I think that all Australians, regardless of where they live, should have access to accurate medical diagnoses and interventions. When it comes to basic access to specialist care in remote and rural locations, the playing field really needs to be levelled.
I read an article in the ABC last year that was talking about people in every state waiting years to see a neurologist. And that’s against a recommended wait time of no more than 30 days. People are not only suffering through their original symptoms for this time, but on top of that we’re finding that they are developing additional complications, often irreversible ones.
I remember reading a similar article a couple of years ago, and things seem to only have gotten worse since then. It’s a problem that is growing and needs new solutions to address it.
What is standing in the way of making this happen? What’s the biggest obstacle you need to solve right now?
All government grants have this kind of roadblock in them, where you need to have a certain amount of data to get this happening in order to get money. But you need money to do the work that gets you the data.
Right now, we need to get our devices in front of vestibular clinicians. They’re the experts; they’re the ones who are in front of patients every day. We need their support in order to take this device further. So, we need the money to manufacture enough devices to send out to these clinicians and then partner with them to do the trials that can give us the data that informs us about how to proceed.
That’s where the support of philanthropy comes in, that’s what gets us across the line and gets us to a point where we have something that says to the government, or a company ‘hey, this is actually possible, this can happen, and now we can pass the baton to you and you can put it out into the world, bring it to the public.’
That’s what we ask for when we ask for people to help us: bridge the gap between what we have now, and what government funding gives us.